
Discussing Endometriosis with Your Daughter
Helping girls navigate puberty and their first periods can be challenging. It’s important to educate all girls about endometriosis, as they may not realize if their experiences are different. Listening to their body-related concerns is crucial.
You can talk to your daughter about endometriosis at any age. It can affect girls as young as 8, so early discussions are important. These conversations create a foundation for more in-depth talks later in life.
The sooner you inform your daughter about endometriosis, the better. Make sure to adapt your communication to her age for better understanding. This helps her grasp that dysmenorrhea, a common symptom in adolescents, can have various causes. This knowledge empowers her to seek help promptly if she ever experiences symptoms of the disease.
Techniques for Alleviating Stress
Coping with the stress of chronic pain associated with endometriosis can be particularly challenging for your daughter. To manage this stress effectively, it’s crucial to foster open communication. This collaborative approach ensures awareness of the challenges your daughter is facing and enables working together to find suitable solutions. Encouraging your daughter to express her feelings and concerns is essential in building a support system that acknowledges the emotional toll of chronic pain.
In addition to communication, incorporating stress-relieving techniques into the daughter’s daily routine is vital. This may include mindfulness exercises, deep breathing, or meditation to help manage both physical and emotional stress. These practices not only provide immediate relief but also empower the teen to take an active role in their well-being.
Moreover, seeking professional support, such as counseling or therapy, can be instrumental in addressing the psychological impact of chronic pain. A mental health professional can assist the teen in developing coping mechanisms, building resilience, and navigating the emotional complexities that often accompany a chronic health condition. It’s essential to recognize that managing stress is a holistic process that involves addressing both the physical and emotional aspects of living with endometriosis.
Methods for your Daughter with Endometriosis to Handle Pelvic Pain While at School
Managing pelvic pain at school can be challenging for your daughter with endometriosis, but there are strategies to help alleviate discomfort:
- Communication with School Staff: Inform teachers and school staff about the condition. They can provide necessary accommodations and understanding during flare-ups.
- Pain Medication: Follow a prescribed pain management plan, which may include taking medication as directed by a healthcare professional. Ensure that the school nurse is aware of any prescribed medications.
- Heat Therapy: Use a heating pad or heat patch on the lower abdomen to alleviate pelvic pain. Consider discreet options that can be easily used during breaks.
- Comfortable Clothing: Wear loose, comfortable clothing to minimize pressure on the abdomen and reduce discomfort.
- Scheduled Rest Breaks: Work with the school to establish a plan for scheduled rest breaks, allowing time to rest and manage pain during the school day.
- Hydration and Nutrition: Stay well-hydrated and maintain a balanced diet. Dehydration and poor nutrition can sometimes exacerbate pain.
- Supportive Friends: Cultivate a supportive network of friends who are understanding and can offer assistance when needed.
- Mindfulness and Relaxation Techniques: Practice mindfulness or relaxation exercises to alleviate stress, which can contribute to pelvic pain.
- Counseling Support: Consider accessing counseling or psychological support to help cope with the emotional impact of chronic pain at school.
It’s essential for teens with endometriosis to collaborate with healthcare professionals and school staff to develop a comprehensive plan that addresses their specific needs. Open communication with teachers and school administrators is key to creating a supportive and accommodating educational environment.
Conversation with Boys in the Family
Initiating conversations about menstruation is not only a vital aspect of a girl’s upbringing but also an essential opportunity to engage boys in understanding this natural process. Educating boys about menstruation is a pivotal step in fostering compassion and empathy, preparing them to comprehend the significant challenges that some girls and women may face.
This knowledge becomes especially valuable as boys grow older, navigating relationships with girlfriends or wives who may encounter difficulties related to menstruation. By breaking down societal taboos and stereotypes through open dialogue, parents empower boys to approach this topic with understanding, contributing to more inclusive and supportive relationships and societies.
Extending these conversations to address conditions like endometriosis is a critical component of family communication. When a daughter is dealing with endometriosis, initiating a dialogue with sons and husbands becomes essential for building a supportive environment.
Encouraging questions and correcting misconceptions ensures that family members are well-informed, equipping them to provide emotional and practical support. By reinforcing the idea that the family plays a crucial role in helping a daughter navigate the challenges of endometriosis, parents foster empathy and support.
How should I handle the situation if my daughter consistently avoids going to school, whether it’s for a single day or multiple consecutive days, due to chronic pain stemming from endometriosis?
If your daughter is consistently refusing to attend school due to chronic pain from endometriosis, it’s crucial to approach the situation with empathy and proactive measures. Firstly, initiate an open and supportive conversation with her. Create a safe space for her to express her feelings and concerns about the pain and its impact on her daily life. Understanding her perspective is essential in finding effective solutions.
Secondly, consult with her healthcare provider to reassess her treatment plan. Ensure that her pain management is optimized and that any necessary adjustments are made to alleviate her symptoms. Discuss the possibility of obtaining a note from her healthcare provider outlining her condition and any necessary accommodations, which can be shared with the school. This can help in facilitating a more understanding and supportive environment for your daughter.
Lastly, collaborate with the school to implement necessary accommodations. Communicate with teachers, counselors, and administrators about her condition, providing information on endometriosis and its impact on her ability to attend regularly. Work together to create a flexible plan that accommodates her needs, such as allowing breaks during the day, providing access to a quiet space, or considering alternative learning options during particularly challenging periods. Regular communication with the school will ensure that everyone is on the same page and working towards the well-being of your daughter.

7 Signs You May Have Endometriosis
Many individuals who menstruate may experience occasional heavy periods, excruciating menstrual cramps, and discomfort during sexual intercourse. However, for up to 10% of females of childbearing age, these symptoms may indicate a more significant issue: endometriosis.
Endometriosis is a medical condition characterized by the displacement of endometrial tissue, which consists of cells resembling the lining of the uterus, outside the uterus, where it adheres to other pelvic organs. These organs can include the fallopian tubes, bladder, or bowels. Each month, during the menstrual cycle, this tissue becomes inflamed and swells, leading to intense pain and, in some cases, infertility.
1. Chronic Pelvic Pain
Endometriosis can result in painful and excessively heavy menstrual periods, but the discomfort doesn’t necessarily cease when your menstruation concludes. Due to the inflammation triggered by endometriosis implants in the pelvic area, pelvic pain can persist as a chronic issue for women affected by this condition.
You might encounter lower abdominal or lower back pain at any point in your monthly cycle. Additionally, endometriosis can lead to discomfort during or after sexual intercourse, as well as pain when urinating or having bowel movements.
2. Heavy Menstrual Periods
Every woman’s menstrual cycle is distinct and personal. What’s considered typical for one woman may not align with the experiences of another. These variations can create uncertainty when trying to discern whether your symptoms may signify a more significant underlying issue.
Experiencing heavy menstrual bleeding is a common concern, yet it shouldn’t be regarded as normal. Heavy bleeding could potentially indicate the presence of endometriosis or another treatable gynecological condition.
You might be dealing with unusually heavy menstrual bleeding if you:
- Witness bleeding persisting for over seven days
- Find yourself changing pads or tampons every hour or even more frequently
- Need to replace pads or tampons during the night
- Pass blood clots that are larger than a quarter
- Experience nausea or vomiting
If these symptoms resonate with your experience, it’s crucial not to delay in scheduling a doctor’s appointment. Heavy menstrual periods are not typical, and seeking medical treatment can have a significant impact on your quality of life.
3. Chronic Lower Back and Abdominal Pain
Persistent lower back and abdominal pain is a symptom commonly associated with endometriosis. This discomfort often occurs throughout the menstrual cycle and may be particularly pronounced during menstruation. The presence of endometrial tissue outside the uterus, leading to inflammation and irritation of surrounding tissues, is thought to be a contributing factor to this chronic pain.
4. Infertility
Endometriosis is a significant factor in female infertility, and it’s essential for young individuals to be aware of this. Many girls discover they have endometriosis when they seek assistance for fertility concerns. Remarkably, up to 50% of women who experience infertility are eventually diagnosed with endometriosis.
Even if you haven’t noticed other typical endometriosis symptoms, it’s crucial to understand that it can still lead to infertility. Endometriosis patches can develop on the ovaries or fallopian tubes, potentially disrupting the processes of ovulation, fertilization, and implantation.
If any of these signs or experiences seem familiar to you, it’s essential to consider the possibility that endometriosis might be a contributing factor. This is a relatively common condition, and there are available treatment options to help improve your symptoms.
5. Painful Bowel Movements or Urination
Experiencing discomfort or pain during bowel movements or urination can be indicative of endometriosis symptoms. In cases of endometriosis, the endometrial tissue that grows outside the uterus, including on or around the pelvic organs, can cause irritation and inflammation. This can lead to pain or discomfort when passing stool or urinating.
6. Irregular Menstrual Cycles
Irregular menstrual cycles can sometimes provide subtle but important hints that something might be amiss, especially for teenagers. While it’s normal for menstrual cycles to vary a bit occasionally, having persistent irregularities could be a signal of an underlying issue. Endometriosis is one such concern—a condition where tissue that resembles the lining of the uterus grows outside the uterus. This can disrupt the typical hormonal and physiological processes of your menstrual cycle, leading to unpredictable or inconsistent patterns.
You might notice unusual cycle lengths or even spotting between your periods. These irregularities might raise suspicion that endometriosis is a possible cause of your menstrual health challenges.
7. Painful Intercourse
Feeling pain during or after sexual intercourse is a common symptom that’s often linked to endometriosis. In endometriosis, tissue that’s similar to the lining of the uterus grows in places it shouldn’t, like around the reproductive organs. When this tissue gets irritated or inflamed, it can cause discomfort or sharp pain when engaging in sexual activities. This can be really distressing and put a strain on the quality of intimate relationships for teens dealing with endometriosis.

Endometriosis Blood in Stool
Rectal endometriosis is a form of endometriosis in which endometrial tissue grows and forms lesions in or on the rectum, often leading to symptoms such as rectal pain, bleeding during bowel movements, and changes in bowel habits. Diagnosis and management of rectal endometriosis typically require a combination of medical evaluation, imaging studies, and, in some cases, surgical intervention to alleviate symptoms and improve the patient’s quality of life.
Is blood in the stool an Endometriosis symptom?
Blood in the stool, while less common, can be a symptom of endometriosis when this condition affects the gastrointestinal tract. Endometriosis can lead to the development of endometrial tissue implants or lesions on or within the rectum and colon, potentially causing rectal bleeding. This bleeding is often more pronounced during menstruation when the endometrial tissue becomes more active. Additionally, endometriosis-related inflammation and scarring in the bowel can result in gastrointestinal symptoms such as abdominal pain, bloating, changes in bowel habits, and discomfort during bowel movements. It’s crucial to note that blood in the stool and gastrointestinal symptoms can also be indicative of other medical conditions, so seeking prompt medical evaluation and diagnosis is essential to determine the underlying cause and appropriate treatment.
If you experience blood in your stool, persistent gastrointestinal symptoms, or any concerning changes in bowel habits, it’s essential to consult a healthcare provider for a comprehensive assessment. They can perform the necessary tests and examinations to identify the cause of your symptoms and provide you with appropriate treatment and management options tailored to your specific condition.
Common Endometriosis Treatment
In cases of endometriosis where there is involvement of the gastrointestinal tract leading to symptoms such as blood in the stool, the treatment approach may involve addressing both the endometriosis and the gastrointestinal symptoms.
Laparoscopic treatment can be used to manage endometriosis by removing endometrial tissue implants and lesions. If there is evidence of endometrial tissue affecting the rectum or colon, the surgeon may carefully excise or ablate these lesions during the laparoscopic procedure.
In addition to the surgical intervention, addressing the gastrointestinal symptoms, including blood in the stool, may require a comprehensive approach. This could involve medications to manage gastrointestinal discomfort, dietary modifications, and lifestyle changes. In some cases, additional consultations with a gastroenterologist may be necessary to evaluate and manage the gastrointestinal component of the condition. It’s important that both the endometriosis and gastrointestinal symptoms are considered and treated appropriately to provide the patient with comprehensive care and symptom relief.
Frequently Asked Question (FAQs)
Is there a cure for endometriosis?
Currently, there is no cure for endometriosis, but there are various treatment options available to manage symptoms. These treatments may include medications, hormonal therapies, lifestyle changes, and surgery. The choice of treatment depends on the individual’s specific circumstances and goals.
What lifestyle changes can help manage endometriosis?
Lifestyle changes that may help manage endometriosis include maintaining a balanced diet, regular exercise, stress reduction techniques, and getting adequate sleep. Additionally, some individuals find relief from symptom exacerbation by avoiding certain foods or triggers that worsen their symptoms. It’s essential to discuss lifestyle modifications with a healthcare provider as part of a comprehensive treatment plan.
Is Deep Infiltrating Endometriosis Life Threatening?
Endometriosis has the capacity to infiltrate nearby organs in close proximity to the uterus, which may encompass the bowel and the urinary bladder. This variant of endometriosis is referred to as “deeply infiltrating” or “deeply invasive endometriosis” (DIE) due to its location deep within the affected tissue or organ.
Fortunately, this occurrence is relatively rare, affecting approximately 1 to 5 percent of women with endometriosis. Treating deeply infiltrating endometriosis can be challenging because it does not consistently respond to medical therapies such as oral contraceptive pills or GnRH agonists.
Is Deep Infiltrating Endometriosis Life Threatening?
Deep infiltrating endometriosis (DIE) itself is generally not considered life-threatening. However, it can significantly affect a person’s quality of life and lead to various health complications. DIE is primarily characterized by its invasion of nearby pelvic organs and tissues, which can result in severe and debilitating pain, particularly during menstruation and sexual intercourse. While not life-threatening in isolation, the persistent pain and its impact on daily functioning can have profound physical and emotional consequences for individuals with this condition.
Although DIE is not inherently life-threatening, it can lead to complications such as fertility problems, as it may affect the fallopian tubes and ovaries. Additionally, it can infiltrate organs like the bowel or urinary bladder, potentially causing issues like bowel or bladder dysfunction. While these complications can have a significant impact on a person’s health and well-being, they can often be managed with medical and surgical interventions. It’s crucial for individuals with DIE to seek medical evaluation and appropriate treatment to alleviate symptoms, improve their overall quality of life, and address any associated health concerns.
Symptoms of Deep Infiltrating Endometriosis
Deep infiltrating endometriosis (DIE) often manifests with a range of distressing symptoms that can greatly impact a person’s quality of life. These symptoms may include severe pelvic pain, typically worsening during menstruation, sexual intercourse, or bowel movements. The pain can be so intense that it disrupts daily activities and may require strong pain medications for management. Additionally, DIE can lead to heavy menstrual bleeding (menorrhagia), chronic pelvic pain that extends beyond the menstrual cycle, and pain during urination or bowel movements. Digestive issues such as bloating, diarrhea, or constipation may occur, particularly when the disease affects the bowel. Fertility problems may also arise, making it difficult for individuals to conceive or leading to recurrent miscarriages, as DIE can affect reproductive organs like the fallopian tubes and ovaries. This complex array of symptoms often necessitates medical attention and tailored treatment.
It’s worth noting that the severity and combination of these symptoms can vary from person to person. Some individuals with DIE may experience only a subset of these symptoms, while others may face multiple severe symptoms that profoundly affect their daily lives. Given the potential impact on health and well-being, individuals experiencing any of these symptoms should seek prompt medical evaluation and consultation with healthcare professionals skilled in the management of endometriosis. Early diagnosis and appropriate treatment can help alleviate suffering, improve quality of life, and address any associated health concerns.
Importance of Laparoscopic Treatment in Deep Infiltrating Endometriosis
Laparoscopic treatment, also known as minimally invasive surgery, plays a crucial role in the management of deep infiltrating endometriosis (DIE) for several important reasons:
- Accurate Diagnosis: Laparoscopy allows for direct visualization of endometriotic lesions, enabling precise diagnosis of the condition. This accuracy is vital in distinguishing DIE from other pelvic conditions and planning appropriate treatment strategies.
- Precise Lesion Removal: Laparoscopic excision surgery enables the targeted removal of endometriotic lesions, including those deeply infiltrating nearby organs. This minimally invasive approach preserves healthy tissue while effectively addressing the root cause of pain and complications associated with DIE.
- Pain Management: Relief from severe pelvic pain is a primary objective in DIE treatment. Laparoscopic surgery offers an effective means of achieving this goal by excising the endometriotic tissue responsible for the pain, improving the patient’s quality of life.
- Fertility Preservation: In cases where fertility is a concern, laparoscopic surgery can help restore normal pelvic anatomy and function. By carefully removing obstructive lesions, laparoscopy can enhance the chances of natural conception, preserving fertility options for affected individuals.
- Minimized Discomfort and Faster Recovery: Laparoscopic procedures involve smaller incisions, resulting in less postoperative pain and faster recovery times compared to open surgery. This minimizes disruption to a patient’s daily life and allows for a quicker return to regular activities.
Phrenic Nerve Endometriosis
Phrenic nerve endometriosis refers to the presence of endometriosis lesions on or near the phrenic nerve. Endometriosis is a condition in which tissue similar to the lining of the uterus, called endometrial tissue, grows outside the uterus. This tissue can implant and grow on various organs within the pelvic region, but in rare cases, it can also affect organs outside the pelvis.
The phrenic nerve is a major nerve that originates in the neck and extends down to the diaphragm, which is the primary muscle responsible for breathing. When endometrial tissue implants on or near the phrenic nerve, it can cause irritation, inflammation, and scarring. This can lead to symptoms such as chest pain, referred shoulder pain, and breathing difficulties.
Phrenic nerve endometriosis is relatively rare, and its exact prevalence is not well-established. It is often challenging to diagnose because the symptoms can mimic other conditions, such as musculoskeletal disorders or respiratory issues. Medical professionals may use a combination of patient history, physical examination, imaging tests (such as magnetic resonance imaging or computed tomography), and in some cases, diagnostic laparoscopy (a minimally invasive surgical procedure) to confirm the presence of endometriosis on the phrenic nerve.
Treatment options for phrenic nerve endometriosis may include a combination of pain management, hormonal therapy (such as birth control pills or GnRH agonists), and surgical intervention. The specific treatment plan depends on the severity of symptoms, the extent of endometriosis involvement, and individual patient factors. It is crucial to consult with a healthcare professional who specializes in endometriosis or a gynecologist for an accurate diagnosis and appropriate management.
Is Phrenic Nerve Endometriosis Life-threatening?
Phrenic nerve endometriosis itself is not typically considered a life-threatening condition; however, it can cause significant discomfort and impact a person’s quality of life due to symptoms such as chest pain and breathing difficulties.
In rare cases, severe involvement of the phrenic nerve and associated complications may require surgical intervention, but with appropriate management, the condition can be effectively treated and managed. It is important to consult with a healthcare professional for an accurate diagnosis and personalized treatment plan.
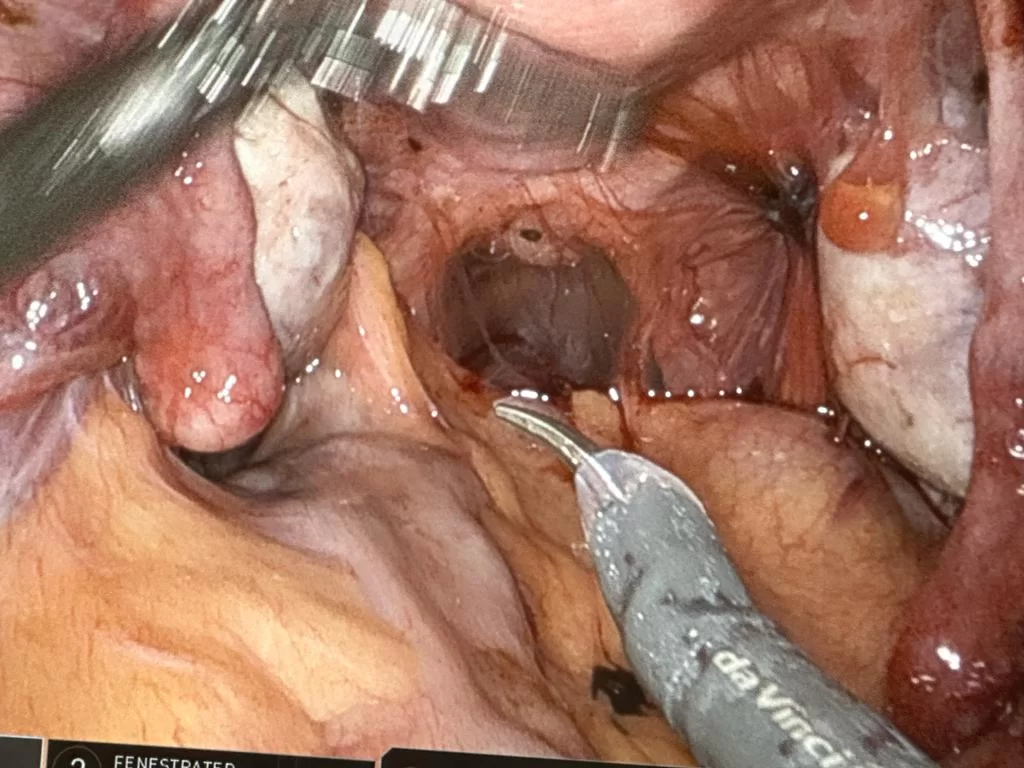
Surgical Treatment for Phrenic Nerve Endometriosis
Surgical treatment for phrenic nerve endometriosis may be considered in cases where conservative measures and medical management have been unsuccessful in relieving symptoms. The specific surgical approach depends on factors such as the extent of endometriosis involvement, severity of symptoms, and individual patient factors.
One surgical option is laparoscopic excision, which is a minimally invasive procedure where the endometriosis lesions are removed using specialized surgical instruments. This approach aims to remove the endometrial implants on or near the phrenic nerve while preserving the surrounding healthy tissue.
In more complex cases or when there is extensive involvement of the phrenic nerve, open surgery may be required. This involves making a larger incision to directly access and remove the endometrial lesions. In some instances, a multidisciplinary team of specialists, including gynecologists and thoracic surgeons, may collaborate to plan and perform the surgery.
The decision to undergo surgery should be made after careful consideration and discussion with a healthcare provider such as New York Gynecology Surgery & Endometriosis (NYGSE) who specializes in endometriosis. They will assess the individual’s specific case, taking into account the severity of symptoms, impact on quality of life, and potential risks and benefits of surgery.
Phrenic Nerve Paralysis After Bipolar Electrocoagulation for Diaphragmatic Endometriosis: A Case Report and Mini-Review
Phrenic nerve paralysis is a rare complication that can occur after bipolar electrocoagulation is used to treat endometriosis of the diaphragm. A case study is presented on this topic by Zippl et al. (2022).
Objective: This report aims to describe a case where the right semi-diaphragm remained elevated after laparoscopic surgery to treat diaphragmatic endometriosis. It suggests that the elevation was likely caused by unintentional damage to important branches of the phrenic nerve due to the use of bipolar electrocoagulation. Additionally, the report provides a brief review of diaphragmatic endometriosis and its surgical treatment options.
Design: This is a case report and mini-review conducted at a single university-based endometriosis center that involves interdisciplinary collaboration.
Patient: The case involves a 33-year-old patient who had not given birth before. The patient initially presented with pain in the right shoulder and back, severe menstrual cramps, and diarrhea. Written consent was obtained to use anonymized data and images for research purposes.
Interventions: The patient underwent laparoscopic surgery, which involved bipolar electrocoagulation of multiple superficial endometriotic lesions on the right semi-diaphragm and excision of deep infiltrating endometriosis on the sacrouterine ligaments bilaterally.
Main outcome measure(s): The main focus was to evaluate the outcomes and complications associated with surgical treatment of diaphragmatic endometriosis.
Results: Three weeks after the surgery, the patient experienced exertional dyspnea (shortness of breath upon exertion) and right flank pain. Imaging revealed that the right semi-diaphragm remained elevated, and this condition persisted for six months. The report suggests that collateral thermal damage to key branches of the phrenic nerve during bipolar electrocoagulation of extensive superficial diaphragmatic lesions may be responsible for these symptoms.
Conclusion(s): The report emphasizes the need for caution when using bipolar electrocoagulation during laparoscopic treatment of diaphragmatic endometriosis to avoid potential damage to the phrenic nerve. It suggests that this technique should be used sparingly and with careful consideration.
Importance of Laparoscopic Treatment
The significance of utilizing laparoscopic treatment lies in its ability to minimize the risk of damaging the phrenic nerve
Laparoscopic treatment for phrenic nerve endometriosis is considered important because it offers several advantages in terms of minimizing potential damage to the phrenic nerve and facilitating a faster recovery.
Laparoscopic procedures are minimally invasive, involving small incisions through which a camera and specialized surgical instruments are inserted. The surgeon can visualize the affected area on a screen and perform precise movements to remove endometrial implants while minimizing trauma to surrounding tissues.
The benefits of laparoscopic treatment include:
- Nerve preservation: Laparoscopic techniques allow for better visualization and precision during surgery, reducing the risk of unintentional damage to the phrenic nerve. The surgeon can carefully navigate and manipulate tissues to preserve nerve integrity.
- Reduced scarring and pain: With smaller incisions, laparoscopic surgery generally results in less scarring and postoperative pain compared to open surgery. This can contribute to a quicker recovery and improved patient comfort.
- Shorter hospital stay: Laparoscopic procedures typically have shorter hospital stays compared to open surgeries, allowing patients to return to their normal activities sooner.
- Quicker recovery: The minimally invasive nature of laparoscopic surgery often leads to a faster overall recovery time, allowing patients to resume their daily routines and activities more quickly.

Misdiagnosis of Endometriosis
Misdiagnosis of endometriosis refers to the situation where a person with endometriosis is given an incorrect diagnosis, usually of another condition, by a healthcare provider. It means that the healthcare provider fails to recognize or correctly identify the presence of endometriosis in the patient.
The misdiagnosis of endometriosis can take various forms. It may involve attributing the symptoms to another physical health condition, such as gastrointestinal issues or urinary tract problems. Additionally, endometriosis may be mistaken for a mental health problem, particularly when symptoms like chronic pain and emotional distress are present.
Endometriosis is often misdiagnosed for several reasons:
- Symptom Overlap: The symptoms of endometriosis can mimic those of other conditions, leading to misdiagnosis. Common symptoms of endometriosis include pelvic pain, heavy or irregular menstrual periods, pain during intercourse, and infertility. These symptoms can also be associated with other gynecological, gastrointestinal, or urinary tract disorders, such as ovarian cysts, irritable bowel syndrome (IBS), or urinary tract infections. The similarity in symptoms can make it challenging to differentiate endometriosis from other conditions.
- Lack of Awareness: Endometriosis historically received less attention and research compared to other conditions, resulting in a lack of awareness among both the general population and healthcare providers. This limited awareness can contribute to a delayed diagnosis or misdiagnosis. Many healthcare professionals may not consider endometriosis as a potential cause of symptoms and may focus on more common conditions, leading to misdiagnosis.
- Diagnostic Challenges: Diagnosing endometriosis definitively requires a surgical procedure called laparoscopy, which involves inserting a small camera into the abdomen to visualize and remove endometrial lesions. However, laparoscopy is an invasive procedure and may not be performed unless endometriosis is strongly suspected. Non-invasive diagnostic methods, such as imaging tests like ultrasound or MRI, cannot reliably detect endometriosis, further complicating the diagnosis process.
- Normalization of Symptoms: Many individuals with endometriosis may consider their symptoms, such as menstrual pain, as a normal part of their menstrual cycle. Similarly, healthcare providers may dismiss symptoms as typical menstrual discomfort, leading to a delay in seeking a diagnosis and contributing to misdiagnosis.
- Bias and Stereotypes: Gender bias and stereotypes can also play a role in misdiagnosis. Endometriosis primarily affects individuals assigned female at birth, and there is a historical tendency to downplay or dismiss women’s pain and reproductive health concerns. This bias can result in healthcare providers attributing the symptoms to psychological factors or generalizing them as “women’s issues,” leading to misdiagnosis or delayed diagnosis.
To address the issue of misdiagnosis, it is important to improve education and awareness about endometriosis among healthcare providers, enhance diagnostic tools and techniques, and promote a more comprehensive and inclusive approach to women’s health, where symptoms are taken seriously and thoroughly investigated to ensure accurate diagnoses.
Perceptions of Endometriosis Misdiagnosis from the Patient’s Perspective
A study conducted by Allyson C Bontempo and Lisa Mikesell in 2020 investigated patient perceptions of misdiagnosis in endometriosis through an online national survey.
Here are the key findings from the study:
- Diagnostic Delay: The average reported diagnostic delay for endometriosis was 8.6 years. This means that, on average, it took 8.6 years for patients to receive a correct diagnosis for their endometriosis.
- Misdiagnosis Rates: 75.2% of patients reported being misdiagnosed with another physical health condition (95.1%) and/or a mental health problem (49.5%). This indicates that the majority of patients initially received incorrect diagnoses before being correctly diagnosed with endometriosis.
- Types of Misdiagnoses: Among the misdiagnosed patients, gynecologists were responsible for misdiagnosing 53.2% of them, followed by general practitioners who misdiagnosed 34.4% of the patients.
- Factors Influencing Misdiagnosis: Several factors were found to be associated with a higher likelihood of reporting a misdiagnosis. These factors include experiencing virtually all symptoms associated with endometriosis and having endometriosis in specific locations such as the bladder, small bowel, pelvic sidewall, and rectum. Additionally, reporting a misdiagnosis of a physical health condition was exclusively associated with endometriosis on the appendix, while reporting a misdiagnosis of a mental health problem was exclusively associated with a younger age of symptom onset, endometriosis on the diaphragm, large bowel, lung, and ureter, as well as having a comorbid diagnosis of adenomyosis.
In summary, this study found that endometriosis diagnosis is often delayed, and a significant proportion of patients are initially misdiagnosed with other physical or mental health conditions. Gynecologists and general practitioners were the most common healthcare providers involved in these misdiagnoses. Various factors, such as symptom profile and the location of endometriosis, were associated with a higher likelihood of misdiagnosis.
New York Gynecology Endometriosis (NYGE) is committed to accurate diagnosis and effective treatment. We understand the challenges associated with misdiagnosis and the impact it can have on patients’ lives. Our highly skilled team, led by Dr Pankaj Singhal, stays up to date with the latest advancements in endometriosis research and treatment options.
By prioritizing thorough evaluations and utilizing state-of-the-art diagnostic techniques, we strive to provide our patients with precise and personalized care. At New York Gynecology Endometriosis, you can trust that your concerns will be heard, and an accurate diagnosis will be reached to guide the most appropriate treatment plan for your individual needs.

Vagus Nerve Endometriosis
Endometriosis involving the vagus nerve is a relatively rare occurrence. The vagus nerve is a large nerve that extends from the brainstem down to the abdomen and plays a crucial role in regulating various bodily functions. While endometriosis typically involves the presence of endometrial tissue outside the uterus, it most commonly affects the pelvic region, including structures such as the ovaries, fallopian tubes, and peritoneum.
Endometriosis affecting the vagus nerve is referred to as “vagal endometriosis” or “extrapelvic endometriosis.” It occurs when endometrial tissue implants on or near the vagus nerve, leading to potential irritation, inflammation, or compression of the nerve. This can result in symptoms such as pain, altered sensation, or dysfunction in areas innervated by the vagus nerve, which includes the throat, chest, digestive tract, and even the heart.
The diagnosis of vagal endometriosis can be challenging due to its rarity and the overlapping nature of symptoms with other conditions. It often requires a comprehensive evaluation, including a thorough medical history, physical examination, imaging studies, and, in some cases, surgical exploration and biopsy to confirm the presence of endometrial implants near the vagus nerve.
Treatment options for vagal endometriosis typically involve a multidisciplinary approach, which may include pain management strategies, hormonal therapies to suppress endometrial growth, and, in some cases, surgical intervention to remove or excise the affected tissue. The specific treatment plan will depend on the individual’s symptoms, the extent of the endometriosis, and the patient’s overall health.
If you suspect vagal endometriosis or are experiencing symptoms involving the vagus nerve, it is important to consult with a healthcare professional who specializes in endometriosis or a relevant specialist, such as a gynecologist or neurologist, for a proper evaluation, diagnosis, and management.
What Trigger Vagus Nerve Endometriosis?
The exact triggers for vagus nerve endometriosis, like endometriosis in general, are not yet fully understood. However, endometriosis is thought to be influenced by several factors, and some of these may potentially contribute to the development of endometriosis near the vagus nerve. These factors include:
- Retrograde menstruation: Retrograde menstruation occurs when menstrual blood containing endometrial cells flows backward through the fallopian tubes into the pelvic cavity instead of being expelled through the vagina. This is considered a common process, and it may play a role in the development of endometriosis in various locations, including near the vagus nerve.
- Hormonal factors: The growth and activity of endometrial tissue are influenced by hormonal fluctuations, particularly estrogen. Abnormal estrogen levels or imbalances may contribute to the development and progression of endometriosis, including in locations near the vagus nerve.
- Genetic factors: There may be a genetic predisposition to endometriosis, and certain gene mutations or variations could potentially increase the risk of developing the condition, including endometriosis near the vagus nerve.
- Immune system dysfunction: Disruptions in the immune system’s response to endometrial tissue outside the uterus may play a role in the development of endometriosis. This dysfunction could potentially contribute to the formation of endometrial implants near the vagus nerve.
It’s important to note that while these factors may be associated with endometriosis in general, the specific triggers for vagus nerve endometriosis have not been extensively studied or identified. Further research is needed to better understand the mechanisms and triggers specific to endometriosis involving the vagus nerve.
Symptoms of Vagus Nerve Endometriosis
Vagus nerve endometriosis is a rare condition, and the symptoms associated with it can vary from person to person. However, since the vagus nerve is involved in regulating numerous bodily functions, including those of the digestive tract, heart, and respiratory system, endometriosis affecting the vagus nerve can potentially cause a range of symptoms. These may include:
- Visceral pain: Visceral pain refers to pain originating from the internal organs. Vagus nerve endometriosis may lead to pain in areas innervated by the vagus nerve, such as the throat, chest, upper abdomen, or deep within the body.
- Dysphagia: Difficulty swallowing or a sensation of food getting stuck in the throat can occur if the vagus nerve’s function is affected by endometriosis.
- Gastrointestinal symptoms: Endometriosis involving the vagus nerve may lead to symptoms such as nausea, vomiting, bloating, abdominal pain, or altered bowel movements.
- Cardiac symptoms: The vagus nerve plays a role in regulating heart function, and endometriosis affecting the vagus nerve could potentially cause symptoms such as palpitations, irregular heartbeats, or changes in heart rate.
- Respiratory symptoms: In some cases, vagus nerve endometriosis may be associated with respiratory symptoms such as difficulty breathing or a feeling of tightness in the chest.
It’s important to note that the symptoms of vagus nerve endometriosis can overlap with other medical conditions, and a comprehensive evaluation by a healthcare professional like the team of New York Gynecology Endometriosis is necessary for an accurate diagnosis.

Proctalgia and Endometriosis
Proctalgia and endometriosis are two distinct medical conditions that affect different areas of the body. Let’s discuss each of them separately:
Proctalgia
Proctalgia, also known as levator ani syndrome, is a condition characterized by recurrent episodes of rectal pain or discomfort. The exact cause of proctalgia is unknown, but it is believed to be related to muscle spasms in the pelvic floor, specifically involving the levator ani muscles. Symptoms may include sharp or cramping pain in the rectum or anus, which can last for several minutes or even hours.
The diagnosis of proctalgia is usually made based on the characteristic symptoms and the exclusion of other possible causes of rectal pain through a medical evaluation. Treatment options for proctalgia focus on relieving symptoms and managing pain during episodes. This may include techniques such as warm baths, relaxation exercises, pain medications, and occasionally muscle relaxants. In severe cases, biofeedback therapy or injections of botulinum toxin into the pelvic floor muscles may be considered.
Proctalgia Fugax
Proctalgia fugax is a relatively common condition characterized by sudden, sharp rectal pain that occurs spontaneously and lasts for a short duration. The term “fugax” comes from the Latin word meaning “fleeting,” which accurately describes the nature of the pain experienced. These episodes of pain can occur at any time, often during the night or early morning, and typically last for a few seconds to a few minutes before subsiding on their own.
It is important to note that in some cases, individuals with endometriosis may also experience symptoms of proctalgia fugax. This could be due to the proximity of endometrial implants to the rectal area, which may cause referred pain or irritation in the rectum. Additionally, endometriosis can involve the infiltration of nerves in the pelvic region, which could contribute to heightened sensitivity and pain sensations.
What Triggers Proctalgia Fugax?
Proctalgia fugax episodes can be triggered by various factors, although the exact cause of the condition is not fully understood. Some common triggers reported by individuals with proctalgia fugax include:
- Muscle spasms: Proctalgia fugax is thought to be caused by spasms of the muscles in the rectal area or pelvic floor. These spasms can be triggered by factors such as muscle tension, overexertion, or straining during bowel movements.
- Stress and anxiety: Emotional stress and anxiety have been known to trigger or exacerbate episodes of proctalgia fugax. Managing stress levels through relaxation techniques or stress-reducing activities may help alleviate symptoms.
- Certain foods and drinks: Some individuals report that certain foods or beverages can trigger episodes of proctalgia fugax. Common triggers include spicy foods, caffeine, alcohol, and carbonated drinks. It can be helpful to keep a food diary to identify any specific triggers in your own case.
- Sitting or postural factors: Prolonged sitting, particularly on hard surfaces, or maintaining certain positions for an extended period may contribute to the occurrence of proctalgia fugax episodes in some individuals. Changing positions regularly and using cushioning or ergonomic support may help prevent or minimize symptoms.
- Hormonal fluctuations: While not well-established, some individuals report that hormonal changes during the menstrual cycle can influence the frequency or intensity of proctalgia fugax episodes. Further research is needed to fully understand this relationship.
It’s important to note that triggers can vary from person to person, and not everyone will have identifiable triggers for their proctalgia fugax episodes. Keeping track of your symptoms and potential triggers can be helpful in managing the condition and discussing it with your healthcare provider.
Endometriosis
Endometriosis is a chronic condition in which tissue similar to the lining of the uterus, called the endometrium, grows outside the uterus. This tissue can implant and grow on various structures within the pelvis, such as the ovaries, fallopian tubes, outer surface of the uterus, and other pelvic organs. Endometriosis is a hormone-dependent condition, meaning it is influenced by the menstrual cycle.
Common symptoms of endometriosis include pelvic pain, painful menstrual periods, pain during sexual intercourse, and infertility. In some cases, endometriosis can also affect the bowel and cause symptoms such as painful bowel movements, diarrhea, constipation, or rectal pain.
The diagnosis of endometriosis often requires a combination of medical history, pelvic examination, imaging studies (such as ultrasound), and sometimes a surgical procedure called laparoscopy to visualize and confirm the presence of endometrial tissue outside the uterus. Treatment options for endometriosis may include pain medication, hormonal therapies (such as birth control pills or gonadotropin-releasing hormone agonists), and in severe cases, surgery to remove the endometrial implants.
While proctalgia and endometriosis can both involve symptoms related to the rectal area, they have different underlying causes and require distinct approaches to diagnosis and management. If you are experiencing any symptoms or concerns, it is important to consult with a healthcare professional for an accurate evaluation and appropriate treatment recommendations.
Similarities of Proctalgia and Endometriosis
Proctalgia and endometriosis are two distinct medical conditions, and their similarities are limited. However, they both involve symptoms that can affect the rectal area. Here are a few general similarities:
Rectal pain: Both proctalgia and endometriosis can cause pain in or around the rectum. In proctalgia, the pain is typically brief and episodic, while in endometriosis, the pain can be chronic and associated with the menstrual cycle.
Impact on quality of life: Both conditions can significantly impact a person’s quality of life. The pain experienced in the rectal area can cause discomfort, interfere with daily activities, and affect emotional well-being.
Diagnostic challenges: Both proctalgia and endometriosis can be challenging to diagnose accurately. Proctalgia fugax, in particular, is a diagnosis of exclusion, meaning other potential causes of rectal pain must be ruled out. Similarly, endometriosis often requires a combination of clinical evaluation, imaging studies, and, in some cases, surgical intervention (laparoscopy) to confirm the presence of endometrial tissue outside the uterus.
Potential overlap: In some cases, individuals with endometriosis may experience symptoms similar to proctalgia fugax, where they may have episodes of rectal pain unrelated to their endometrial implants. However, this overlap is not universal and does not imply a direct causal relationship between the two conditions.

Signs and Symptoms of Endometriosis
What are the First Signs of Endometriosis?
- Painful menstrual periods (dysmenorrhea): Severe menstrual cramps that may begin one or two days before menstruation and last for several days. The pain may be located in the lower abdomen, back, or pelvis.
- Pelvic pain: Chronic or recurring pelvic pain that occurs outside of the menstrual period. It may be described as a dull, aching pain or sharp, stabbing pain.
- Pain during or after sexual intercourse (dyspareunia): Deep pelvic pain during or after intercourse. This pain may persist for some time after sexual activity.
- Painful bowel movements or urination: Pain or discomfort during bowel movements or urination, especially during menstruation. This can be accompanied by diarrhea, constipation, bloating, or blood in the urine.
- Heavy or irregular menstrual bleeding: Menstrual periods that are abnormally heavy or longer than usual. Some women may also experience spotting between periods.
- Fatigue: Excessive tiredness or low energy levels, which may be attributed to the chronic pain and inflammation associated with endometriosis.
Uncommon Symptoms of Endometriosis
- Digestive issues: Some individuals with endometriosis may experience symptoms such as bloating, constipation, diarrhea, or nausea, especially during their menstrual cycle.
- Urinary symptoms: Endometrial implants on the bladder or urinary tract can lead to urinary urgency, frequent urination, or blood in the urine.
- Lower back or leg pain: In rare cases, endometriosis can cause lower back pain or radiating pain down the legs, similar to sciatica.
- Painful bowel movements or bleeding from the rectum: Endometrial implants on or near the rectum can cause pain during bowel movements and, in rare instances, rectal bleeding.
- Chest pain or shortness of breath: A very rare form of endometriosis, called thoracic endometriosis, can affect the lungs or chest cavity, causing symptoms such as chest pain or difficulty breathing.

21 Myths and Facts About Endometriosis
Endometriosis affects approximately 1 in 10 American women, making it a prevalent condition that is often misunderstood. It involves the abnormal growth of tissue similar to the uterine lining, known as the endometrium, outside of the uterus. These growths can lead to pain, scarring, and even infertility.
Unfortunately, a woman with endometriosis may go undiagnosed for up to seven years due to symptoms that resemble other common conditions like irritable bowel syndrome or pelvic inflammatory disease. Moreover, misconceptions surrounding the disease contribute to the hesitance of some women to seek medical assistance. To address concerns about painful periods or persistent pain in the lower back or pelvis, it is crucial to engage with your healthcare team for appropriate support and guidance.
Top 21 Myths and Facts About Endometriosis
Myth 1: Symptoms are merely attributed to heavy menstrual periods.
Some women with endometriosis mistakenly believe that their symptoms are typical for menstruation, and when they do seek help, they may be dismissed as overreacting to normal menstrual discomfort. However, the reality is that something far more significant is occurring beyond regular period cramps. One hypothesis suggests that the pain arises because even when endometrium-like tissue exists outside the uterus, it remains responsive to hormonal signals and releases chemicals that trigger inflammation and pain.
Throughout the menstrual cycle, this displaced endometrium-like tissue thickens and eventually undergoes bleeding. Unlike endometrial tissue within the uterus that can be expelled through the vagina each month, blood from the displaced tissue lacks an exit route. Consequently, it accumulates near the affected organs and tissues, causing irritation and inflammation. The outcome is persistent pain and, in some cases, the formation of adhesive scar tissue that can intertwine organs, resulting in discomfort during movement or sexual activity.
Myth 2: Endometriosis solely impacts the pelvic area.
While the pelvis, including the outer surface of the uterus, bladder, and fallopian tubes, is the most frequently affected region by endometriosis growths, it is important to recognize that endometriosis can develop anywhere in the body. In rare cases, endometrium-like tissue has even been identified in unexpected locations such as the lungs.
Myth 3: Endometriosis is universally characterized by pain.
Contrary to popular belief, not all individuals with endometriosis suffer from pain. In some cases, a woman may discover she has endometriosis only when investigating fertility challenges. It is worth noting that endometriosis is a leading cause of infertility in the United States and can elevate the risk of miscarriage and other pregnancy complications. However, it is encouraging to know that the majority of women with endometriosis eventually achieve the ability to conceive and have a child.
Myth 4: Endometriosis is preventable.
Due to the lack of a definitive understanding of the cause of endometriosis, there are no known methods to prevent its occurrence. However, taking certain measures to lower estrogen levels in the body can help decrease the risk, as estrogen can contribute to the growth of endometriosis and intensify symptoms. According to the US Office of Women’s Health, opting for a lower-estrogen birth control method, maintaining a healthy weight, and engaging in regular exercise are ways to reduce estrogen levels. While these steps may mitigate the risk, they do not guarantee the prevention of endometriosis.
Myth 5: Endometriosis always improves after menopause.
While endometriosis symptoms predominantly manifest during menstruation, some women continue to experience them even after the cessation of monthly cycles. This is because, after menopause, the ovaries still produce small quantities of estrogen.
Endometriosis growths may persistently respond to this hormone, leading to ongoing pain. Although many women witness an improvement in endometriosis symptoms after menopause, it is important to note that not all individuals experience relief. In some cases, women who have undergone menopause may opt for surgical interventions, such as the removal of endometriosis implants or adhesions, or even a hysterectomy and oophorectomy (ovary removal). However, it is crucial to recognize that these procedures do not guarantee pain control. Additionally, hormonal therapies appear to be less effective in managing endometriosis symptoms in women who have reached menopause.
Myth 6: Only older women can have endometriosis.
Endometriosis can develop in women of any age, including teenagers and young adults. While the condition is commonly diagnosed in individuals during their reproductive years, it is not limited to a specific age group.
Endometriosis can present itself shortly after a person’s first period and persist throughout their reproductive life. It is crucial to be aware of potential symptoms and seek medical attention regardless of age if there are concerns about endometriosis. Recognizing the misconception that only older women can have endometriosis is essential to ensure timely diagnosis and appropriate management for individuals of all age groups affected by this condition.
Myth 7: Endometriosis is just a women’s issue.
This belief overlooks the broader impact of endometriosis beyond the individual experiencing it. While it is true that endometriosis primarily affects people assigned female at birth, it can have significant effects on their partners, families, and support networks.
The physical and emotional challenges posed by endometriosis can influence various aspects of a person’s life, including their relationships, mental well-being, and overall quality of life. Partners and family members may also be affected as they provide support and witness the impact of the condition on their loved ones.
Moreover, endometriosis can have socioeconomic implications, such as missed work or educational opportunities, financial burdens due to medical expenses, and the need for specialized healthcare.
Myth 8: Endometriosis is always accompanied by visible symptoms.
Endometriosis is a complex condition that can manifest differently in different individuals.
While some people with endometriosis may experience noticeable symptoms such as pelvic pain, painful periods, or infertility issues, others may have no apparent external signs or visible indications of the condition. In fact, there are cases where individuals may have extensive endometriosis with minimal or no symptoms at all. This makes it challenging to diagnose endometriosis based solely on visible manifestations.
It is important to note that the severity of symptoms does not necessarily correlate with the extent or stage of the condition. Some individuals with mild endometriosis may experience severe pain, while others with extensive endometriosis may have minimal discomfort.
Myth 9: Women with endometriosis cannot get pregnant.
While endometriosis can affect fertility, it does not mean that all women with endometriosis are unable to conceive. It is important to understand that fertility is variable and can differ among individuals with endometriosis.
Many women with the condition are able to conceive naturally or with medical interventions. With appropriate management, including fertility treatments and assisted reproductive technologies, such as in vitro fertilization (IVF), the chances of pregnancy can be improved for individuals with endometriosis.
Myth 10: Pregnancy and childbirth will cure endometriosis.
While it is true that some individuals may experience temporary relief from endometriosis symptoms during pregnancy, as the hormonal changes can suppress the growth of endometrial tissue, it does not provide a permanent cure for the underlying condition. Endometriosis is a chronic condition that involves the presence of endometrium-like tissue outside the uterus, and it requires appropriate management and treatment.
After childbirth, endometriosis can potentially resume or persist, as the hormonal fluctuations postpartum can trigger the regrowth of endometrial tissue and reactivation of symptoms. In some cases, symptoms may even worsen after pregnancy.
Myth 11: Surgery always cures endometriosis.
The myth suggests that surgery is always a guaranteed cure for endometriosis, implying that undergoing a surgical procedure will completely eliminate the condition and its symptoms. However, this is not entirely true.
Surgery can be an effective treatment option for endometriosis, particularly in cases where there are visible endometrial implants, adhesions, or cysts that can be excised or removed. The surgical procedure commonly used for endometriosis is called laparoscopy, where a thin tube with a camera is inserted through small incisions in the abdomen to visualize and address the affected areas.
While surgery can provide relief and improvement in symptoms for many individuals, it does not guarantee a permanent cure. Endometriosis is a chronic condition that involves the presence of endometrial-like tissue outside the uterus, and it can be challenging to completely eradicate all affected areas during surgery. Additionally, there is a possibility of disease recurrence or new endometrial growths developing over time.
Myth 12: Endometriosis is a rare condition.
Endometriosis is actually a common condition that affects a significant number of people, particularly those assigned female at birth.
Endometriosis is estimated to impact as many as 1 in 10 individuals assigned female at birth, which translates to a substantial portion of the population. It is one of the most prevalent gynecological disorders, affecting millions of people worldwide. Despite its prevalence, endometriosis often remains underdiagnosed or misdiagnosed due to various factors such as lack of awareness, symptom variability, and the normalization of menstrual pain.
Myth 13: Hysterectomy is a cure for endometriosis.
While a hysterectomy (removal of the uterus) can alleviate symptoms associated with endometriosis, it is not a cure. Endometriosis can still persist in other areas outside the uterus, and symptoms may continue.
Myth 14: Endometriosis is just a psychological condition.
Endometriosis is a medical condition with physical manifestations. It is not a psychological disorder. The pain and other symptoms experienced by women with endometriosis are real and not imagined.
Myth 15: Hormonal birth control always treats endometriosis effectively.
Hormonal birth control methods, such as oral contraceptives, can help manage endometriosis symptoms for some women. However, they may not be effective for everyone, and different treatments may be necessary to find the most suitable approach for each individual.
Myth 16: Endometriosis is caused by poor hygiene or sexual promiscuity.
Endometriosis is not caused by uncleanliness, sexual activity, or promiscuity. The exact cause of endometriosis is unknown, but it is believed to involve a combination of genetic, hormonal, and immune system factors.
Myth 17: Women with endometriosis should avoid exercise.
Exercise can actually be beneficial for women with endometriosis. It can help reduce pain, improve overall well-being, and promote healthy circulation. However, it’s important to listen to your body and avoid activities that worsen your symptoms.
Myth 18: Endometriosis is only diagnosed through invasive surgery.
While laparoscopic surgery is the gold standard for diagnosing endometriosis definitively, it is not always the first step. A thorough medical history, pelvic examination, and imaging techniques such as ultrasound or MRI can provide valuable information.
Myth 19: Endometriosis is a form of cancer.
Endometriosis is not a type of cancer and should not be confused with malignant or cancerous conditions.
Endometriosis is a chronic gynecological disorder where tissue similar to the lining of the uterus, called the endometrium, grows outside of the uterus. While endometriosis can cause pain, inflammation, and adhesions, it is a non-cancerous condition.
Cancer, on the other hand, is characterized by the uncontrolled growth and spread of abnormal cells in the body. Cancer cells invade nearby tissues and can metastasize to other organs. Unlike endometriosis, cancer poses significant health risks, including the potential for life-threatening complications.
Myth 20: Endometriosis is a temporary condition that goes away on its own.
Endometriosis is a chronic condition that typically persists unless it is actively managed or treated. It does not resolve spontaneously without intervention.
While the severity of symptoms can fluctuate over time, endometriosis does not typically disappear without treatment. It is a chronic condition that may require long-term management to alleviate symptoms, improve quality of life, and prevent further complications.
Myth 21: Endometriosis only affects the reproductive organs.
The myth suggests that endometriosis is limited to affecting only the reproductive organs, insinuating that the condition exclusively impacts the uterus, ovaries, fallopian tubes, and related structures. However, this is not entirely accurate. While endometriosis commonly affects these reproductive organs, it can also extend beyond them, potentially impacting other areas of the body.
In reality, endometriosis can be found in extrapelvic locations, such as the bowel, bladder, and even distant sites like the lungs or surgical scars. These endometrial-like growths can cause symptoms and complications specific to the affected organs. For example, endometriosis in the bowel can lead to gastrointestinal issues, including abdominal pain, bloating, and digestive disturbances.
Stay updated on our Pinterest account for NYGE and NYGS.