What is Vaginal Cancer?
Cancer is a condition characterized by uncontrolled cell growth within the body. It is typically named after the specific area where it originates, even if it eventually spreads to other parts of the body.
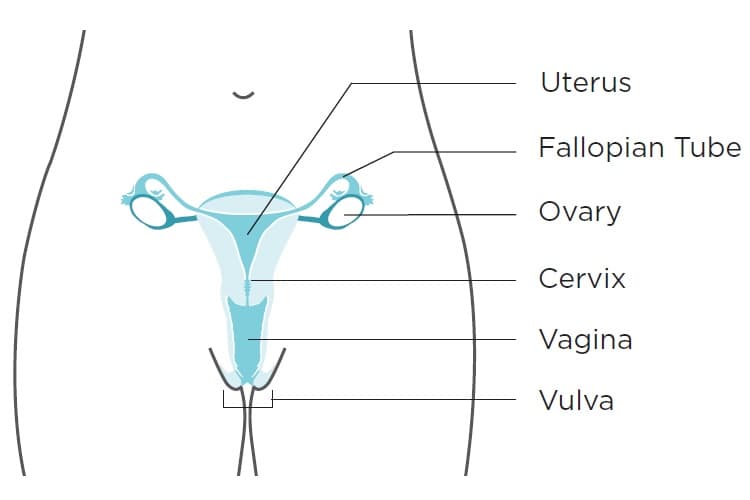
When cancer originates in the vagina, it is referred to as vaginal cancer. The vagina, also known as the birth canal, serves as the passage for menstrual blood and childbirth. It is connected to the cervix, the opening of the uterus, and surrounded by folds of skin known as the vulva.
Under normal circumstances, the vagina remains collapsed with its walls touching. However, during sexual intercourse and vaginal childbirth, the vaginal walls can expand due to numerous folds. The vaginal lining stays moist through mucus released from glands in the cervix.
The vaginal walls consist of a thin layer of cells known as the epithelium, containing squamous epithelial cells. Below the epithelium, the vaginal wall is composed of connective tissue, involuntary muscle tissue, lymph vessels, and nerves.
 Vaginal cancer is an extremely uncommon occurrence. While all women face some risk of these cancers, the likelihood of developing them is very low. Together, vaginal cancers account for approximately 7% of all gynecologic cancers diagnosed in the U.S.
Vaginal cancer is an extremely uncommon occurrence. While all women face some risk of these cancers, the likelihood of developing them is very low. Together, vaginal cancers account for approximately 7% of all gynecologic cancers diagnosed in the U.S.
Approximately 85% of vaginal cancer cases actually stem from cancer that has spread from other parts of the body, with about half of these originating from the cervix or uterus.
Types of Cervical Cancer
Symptoms of Vaginal Cancer
Causes of Vaginal Cancer
Lower Your Chance of Getting Vaginal Cancer
Detection of Vaginal Cancer
Stages of Vaginal Cancer
Stage 1
Stage 1 vaginal cancer indicates that the cancer has begun to grow into the vaginal wall but has not spread beyond that point.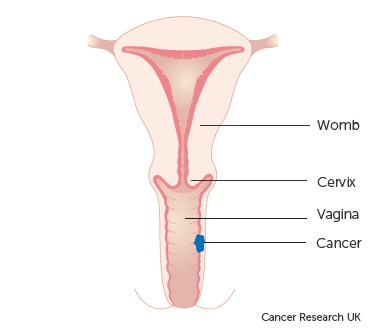
This stage is further divided into two groups:
- Stage 1A: The cancer is localized solely within the vagina and is not larger than 2cm in size. Additionally, it has not spread to nearby lymph nodes close to the vagina.
- Stage 1B: The cancer is confined to the vagina, but it measures more than 2cm in size. Similar to Stage 1A, it has not spread to lymph nodes in the vicinity of the vagina.
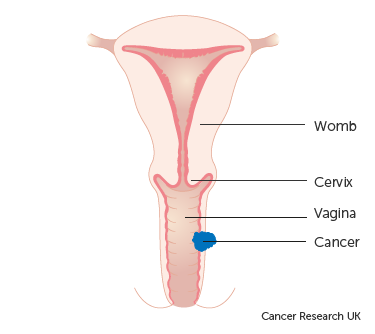
Stage 2
This stage is categorized into two groups:
- Stage 2A: In this stage, the cancer has extended beyond the confines of the vagina into the surrounding tissues. However, it has not reached the walls of the pelvis or nearby lymph nodes. Additionally, the size of the cancer is not larger than 2cm.
- Stage 2B: Similar to Stage 2A, the cancer has spread beyond the vagina into the surrounding tissues without reaching the walls of the pelvis or nearby lymph nodes. However, in this case, the size of the cancer is larger than 2cm.
Stage 3
At this stage, the cancer has advanced beyond the vaginal area and infiltrated the side walls of the pelvis. Consequently, this can lead to urinary difficulties, such as experiencing pain or noticing blood during urination. Additionally, cancer cells might be detected in the lymph nodes located near the vagina.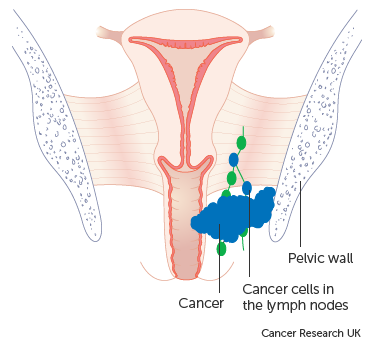
Stage 4
This stage indicates advanced vaginal cancer, signifying that the cancer has metastasized to organs beyond the vagina.
Stage 4 is further divided into two groups:
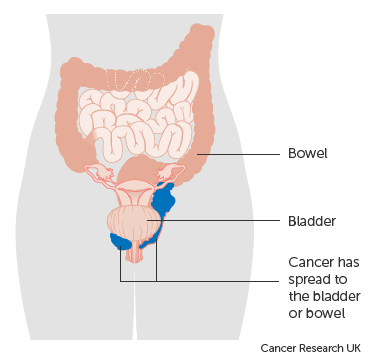
- Stage 4A: In this group, the cancer has spread to other organs, such as the bladder or rectum (back passage).
Stage 4B represents an advanced condition where the cancer has extended to distant organs, such as the lungs or bones.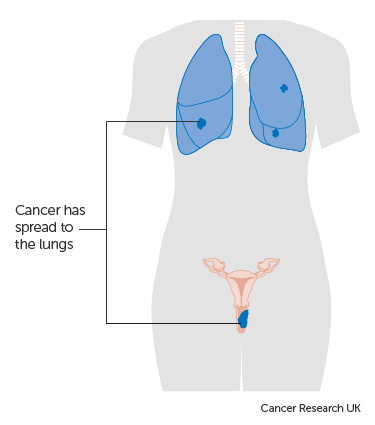
Treatment of Vaginal Cancer
Types of Treatment
NYGSE Approach
